No matter which modality we are using, no matter whether we are practicing screening or diagnostic mammography, no matter what: We still have to position our patients so that all the breast tissue is demonstrated.
That is always a challenge and all the help that comes our way is useful. Here are some tips regarding positioning dilemmas with some handy remedies. I hope they are helpful.
THE CC PROJECTION: “IF”
A. The nipple is not in profile
If the nipple is not in perfect profile:

- Elevate the IMF a little higher
- Lift and pull the breast straight onto the bucky
- Use both hands to handle the breast
- (Hint): The nipple points toward the missing tissue
If the medial cleavage is not visualized properly:
- Position from the medial side
- Lift and drape opposite breast over the edge of the bucky
- Do not press the patient’s face against the face protector
- Place her head beside and beyond the tube

If the lateral aspect of the breast is not seen:
- The Patient’s arm should be relaxed by side
- Her palm should be supinated with her shoulder externally rotated
- Control your patient’s posture with your hand around her back on her contra-lateral shoulder
- She should be relaxed forward bent slightly at the waist
- Release the breast to the compression with forward and medial orientation of your hand
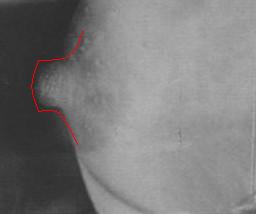
D. The pectoral shadow is not visible at the chest wall and/or the PNL is not within 1cm of the PNL on the MLO

If the ½ moon of pectoral shadow is not seen at the chest wall of the CC view and/or the PNL is of an inadequate length:
A. The pectoral muscle is not demonstrated to or below the level of the nipple
- Elevate the IMF until the tissue no longer moves easily along the chest wall
- Identify the edge of the pectoral muscle visible just under the clavicle
- Loosen the skin over the clavicle so the tissue moves easily
- Compress parallel to the pectoral edge just under the clavicle
- Release hand in a forward medial motion
A. The pectoral muscle is not demonstrated to or below the level of the nipple
If the pectoral muscle is not seen to the level of the nipple or below:

- Adjust your tube angle parallel to the obliquity of the patient’s pectoral muscle
- Move the breast medially and anteriorly from the lateral border until the pectoral pouches out next to the sternum
- Compress the projection parallel to the pectoral axis along the sternal edge
If the pectoral shadow does not appear convexly shaped:
- DO NOT rest your patient’s arm along the top edge of the bucky
- Patient’s shoulder should be open, relaxed
- The corner of the bucky high up and well back in the axilla
- Patient’s arm should be slightly bent hanging loosely down the back of the bucky
- Relaxed hand…NO gripping the handle

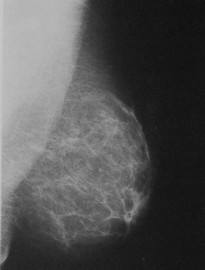
If the retro mammary space is obscured by parenchyma and the breast is not adequately ‘up & out’:
- Move the breast from the lateral edge medially
- Ensure the breast mound moves freely in your grip
- Support the breast tissue from the inferior border using you entire hand
- Immobilize the breast tissue on the bucky in the ‘up & out’ position using the edge of your hand to support the pectoral axis along the sternum
- Release the breast to compression with a distinct out and away motion
If the IMF is not open and fold free:
- Support the breast and always release with and up & out motion
- Have the patient tilt her hips slightly backwards
- Do not release your hold on the breast until the projection is immobilized by the compression
- Gently run your thumb and finger down behind the breast along the IMF/belly border to clear folds, wrinkles and tummy
If the nipple shadow is not in perfect profile:
SUMMARY- Make sure the patient’s feet are directly facing the bucky
- Control the breast from the mobile lateral border only
- Immobilize the breast parenchyma parallel to the pectoral muscle until the compression holds the projection
- (Hint): The nipple points toward the missing tissue
Mammography is a sensitive, complicated and difficult specialty. All our patients vary as to body habitus, temperament and compliance. It is essential we demonstrate all the tissue, see it clearly and know that all the borders of the breast are verified.
Breast Imaging is an area of DI where we work autonomously much of the time. We are responsible for checking and correcting our own work. I send this article once a year for those who have lost theirs or those who are new to techtalk, I hope they will lend a hand in the arduous task of perfecting your technique and knowledge.


No comments:
Post a Comment